
The Future of Equitable Innovation in Healthcare: A Call to Action from Dr. Bayo Curry-Winchell
At a time of transformative potential in healthcare, it’s vital we ask ourselves not just what innovation can do, but whom it will serve. In a powerful and urgent speech, Dr. Bayo Curry-Winchell, president of the Commonwealth Fund and a practicing primary care physician, laid out a compelling blueprint for equitable innovation in healthcare. Speaking from both professional expertise and lived experience, she challenged innovators, policymakers, and clinicians to align the momentum of technological change with the mission of health equity.
This article summarizes the key themes of her message: what are the most pressing issues around equity and innovation, why they matter to all of us, and how each of us—whether we’re technologists, clinicians, funders, or patients—can contribute to building a future where innovation uplifts everyone.
From the Bronx to the Boardroom: A Journey Rooted in Equity
Dr. Curry-Winchell’s career spans more than two decades of clinical work at Mass General Hospital, service in public institutions like NewYork-Presbyterian, and most recently, national leadership as president of the Commonwealth Fund. Her path has been shaped by personal and professional commitment to the underserved—starting in New York and Puerto Rico and extending to the frontlines of the COVID-19 pandemic. That crisis, she recalled, was both the worst of times and the best—marked by urgency, clarity, and a collective push to cut through red tape to save lives.
Her role today is to lead a “think and do” tank founded in 1918 with a mission to advance health for all people. The Commonwealth Fund’s legacy includes funding the country’s first public health departments, rural hospitals, and cervical cancer screening research. Its work today continues to focus on health coverage, cost, care delivery, and international benchmarking—with equity as the guiding principle across all its efforts.
Why the U.S. Healthcare System Is Struggling—Despite Innovation
Despite spending more than any other high-income country, the U.S. ranks last among its peers in health outcomes. Life expectancy is lower. Rates of chronic disease, maternal mortality, and infant mortality are higher. And significant disparities persist across race, geography, income, and gender.
Why? Dr. Curry-Winchell outlined several key drivers:
Underinvestment in social determinants of health: Compared to peer nations, the U.S. invests far less in essentials like education, housing, transportation, and food security—factors that significantly impact health outcomes.
Lack of universal coverage: Other countries have figured out that aligning financing with prevention makes health systems more sustainable. In the U.S., fragmented payment models disincentivize preventive care because the entity making the investment rarely reaps the long-term savings.
Neglect of primary care: The U.S. allocates just 4-5% of its healthcare dollars to primary care, compared to 14-15% in many peer nations. This weakens the foundation of the entire system.
These shortcomings aren’t just policy failures—they’re moral and strategic failures too. And they will be amplified, not diminished, in the coming wave of technological advancement.
Innovation Alone Won’t Fix Equity—Unless We Design for It
There is no doubt we are entering a period of exponential technological growth. From artificial intelligence and remote monitoring to virtual care and wearable diagnostics, the possibilities are astounding. But, Dr. Curry-Winchell cautioned, if equity isn’t built into innovation from the start, the benefits will accrue primarily to those who already have access.
Two significant challenges stand in the way:
Tech diffusion lag: New tools often reach underserved communities last, if at all. This exacerbates disparities rather than closing them.
The digital divide: While broadband and device access have improved, significant gaps remain, especially in rural areas and marginalized urban communities.
Worse, many technologies are being built on data sets and algorithms that contain embedded biases. One example: the pulse oximeter, a common tool in hospitals, has been shown to underperform in patients with darker skin. If we do not actively check for these biases and build tools that work for everyone, inequities will persist in new, more insidious forms.
Why This Matters to All of Us
It’s easy to think of equity as a side issue, or something only relevant to policy experts. But Dr. Curry-Winchell made a forceful case: inequity is inefficient, expensive, and unsustainable. It drives up costs, worsens outcomes, and erodes trust.
Right now, several concurrent crises underscore this:
Coverage is at risk: While 93% of Americans currently have coverage—the highest rate in history—recent political debates threaten to unwind Medicaid expansions and the Affordable Care Act.
Affordability is declining: Even insured individuals are struggling with out-of-pocket costs, deductibles, and premiums that force them to choose between healthcare and daily needs like food or housing.
Access is shrinking: Wait times for primary care appointments are growing in cities like Boston, and many patients simply can’t find a doctor. This isn’t just about location—it’s about workforce.
The primary care workforce is shrinking: From 2012 to 2020, 10% of the workforce left the field. In just one year, from 2021 to 2022, we lost 16,000 more. And with average provider ages climbing, the pipeline is thinning.
Clinician morale is low: Burnout is at an all-time high, driven not only by emotional fatigue but also by a return to overwhelming administrative burdens post-COVID.

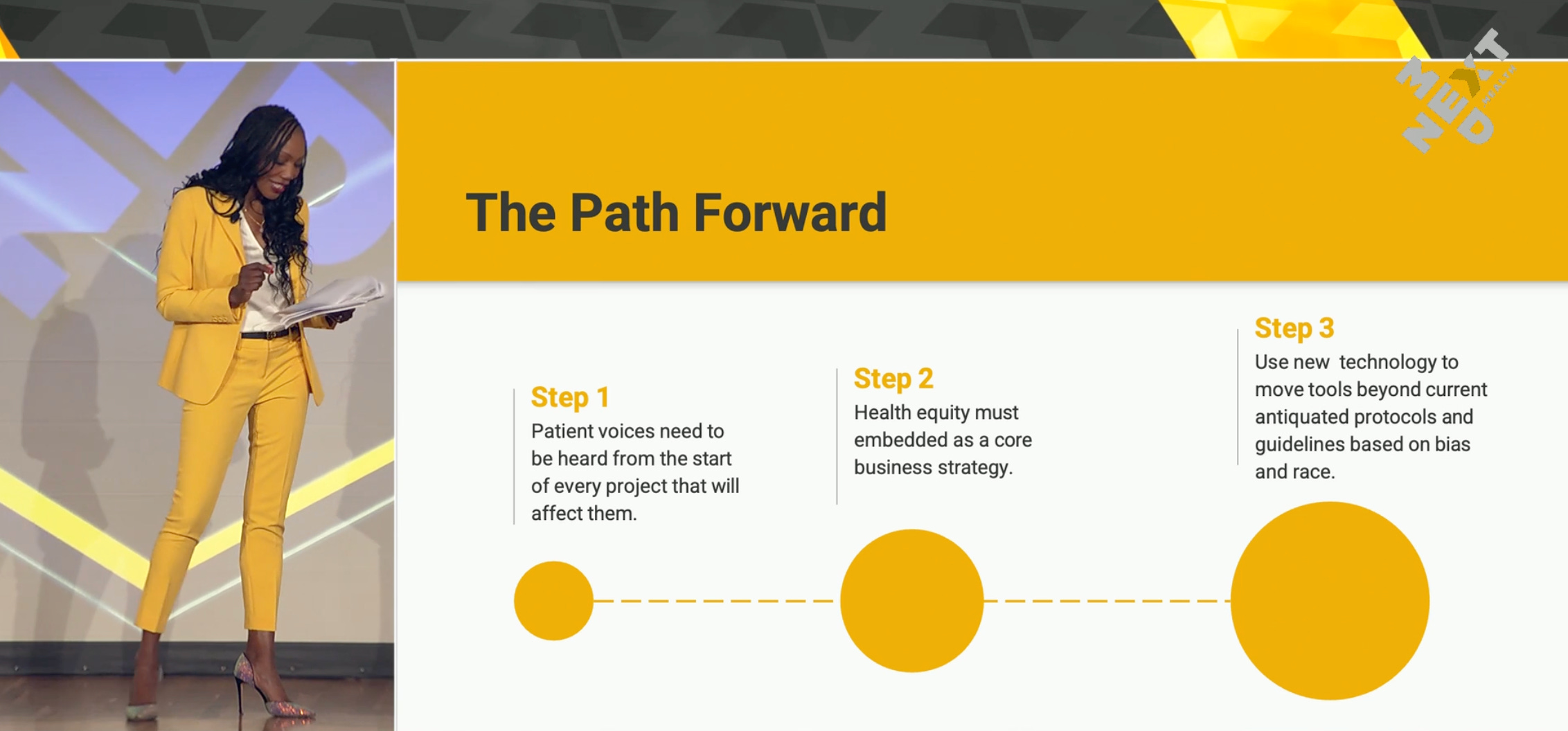
What You Can Do—A Blueprint for Equitable Innovation
As sobering as these challenges are, Dr. Curry-Winchell’s message was ultimately one of hope. “You are incredible innovators,” she told the audience. “So what can you do?” She laid out a framework centered around three pillars: financing, integration, and democratization.
1. Financing Innovation for Equity
Right now, many tools and treatments are available only to those who can pay. GLP-1 medications for diabetes and weight loss, for example, are often out of reach for low-income patients despite being most needed by them. We need new financing models—public, private, or blended—that scale innovation in ways that reach those who need it most.
2. Integrating Technology Into Practice
Many promising tools never make it out of the innovation “graveyard” because we haven’t solved for integration. Clinicians need time, training, and resources to experiment with these tools in their workflows. As Dr. Curry-Winchell noted, “Change is hard when you already have a way of working.” Giving clinicians protected time to explore new tools is critical to successful adoption.
3. Democratizing the Benefits
Innovation must be accessible not just to the digitally savvy elite, but to patients of all backgrounds. That means ensuring language access, designing for cultural competence, and testing tools in diverse settings from the beginning.
Examples of Progress—and What’s Still Missing
Dr. Curry-Winchell shared a powerful example from her own hospital, Mass General, where the system is partnering with Best Buy to scale remote care. The idea: use the Geek Squad to install remote monitoring devices in patients’ homes. It’s smart, scalable, and patient-centered. But it’s not yet coordinated or democratized—and until we fix the financing and integration models, its reach will remain limited.
“We don’t have a shortage of innovation,” she said. “We have a shortage of deployment.”
A Final Plea: Be Proactive About Equity
Dr. Curry-Winchell closed not with critique but with a challenge. Let’s not wait to correct inequities after the fact. Let’s build equity in from the beginning. That means:
Using AI to bridge the language divide in clinical encounters, creating more meaningful patient connections.
Deploying multilingual and multicultural chronic care tools that build trust in marginalized communities.
Creating AI avatars and navigators that improve cancer screening rates and make care more navigable for patients.
Designing solutions for rural and underserved urban communities, where gaps in access are greatest.
Equity is not an add-on. Equity is high-quality care. And it must be the foundation on which we build the future of healthcare innovation.

Conclusion: The Future Must Benefit Everyone
As we race ahead into a future defined by AI, digital diagnostics, and home-based care, we must ask: Who is being left behind? And how do we bring them along?
Dr. Curry-Winchell closed with this call to action: “Let’s ensure that the future we are building—this future of extraordinary promise—truly benefits everyone.”
It’s not enough to build smarter tools. We must build a smarter, more just system.